Foot Capture/Casting/Scanning
Creating a custom-made foot orthosis is an involved process that includes capturing a three-dimensional foot shape, an orthosis design process, and a manufacturing stage. The design and manufacture of an orthosis are performed to the specifications detailed by the foot care professional who performed the full clinical assessment, biomechanical examination, gait analysis, and who casted or scanned the foot. While technology and computer programs are used regularly throughout the fabrication process, it is imperative that the assessing clinician or fabrication technician provide the input to control the design and manufacture of the orthotic device and, as such, must be certified and trained in the relevant technologies.
The following procedures describe the steps in the manufacture of custom foot orthoses:

Foot Capture/Casting/Scanning:
The cast is the medium by which foot structure and position are captured. A cast is a physical or digital model that accurately captures the anatomy and contours of the plantar aspect of the foot while it is in a non-weight bearing, semi-weight-bearing, or full-weight-bearing position. This model must be three-dimensional in order to fabricate a custom-made orthosis for the patient.
Acceptable techniques that may be used to acquire a foot cast used in orthoses manufacturing are manual casting (1) (plaster or sock slipper casting, foam box casting, wax slipper casting, and raw material direct-to-foot moulding), contact digitizing, and optical laser scanning.
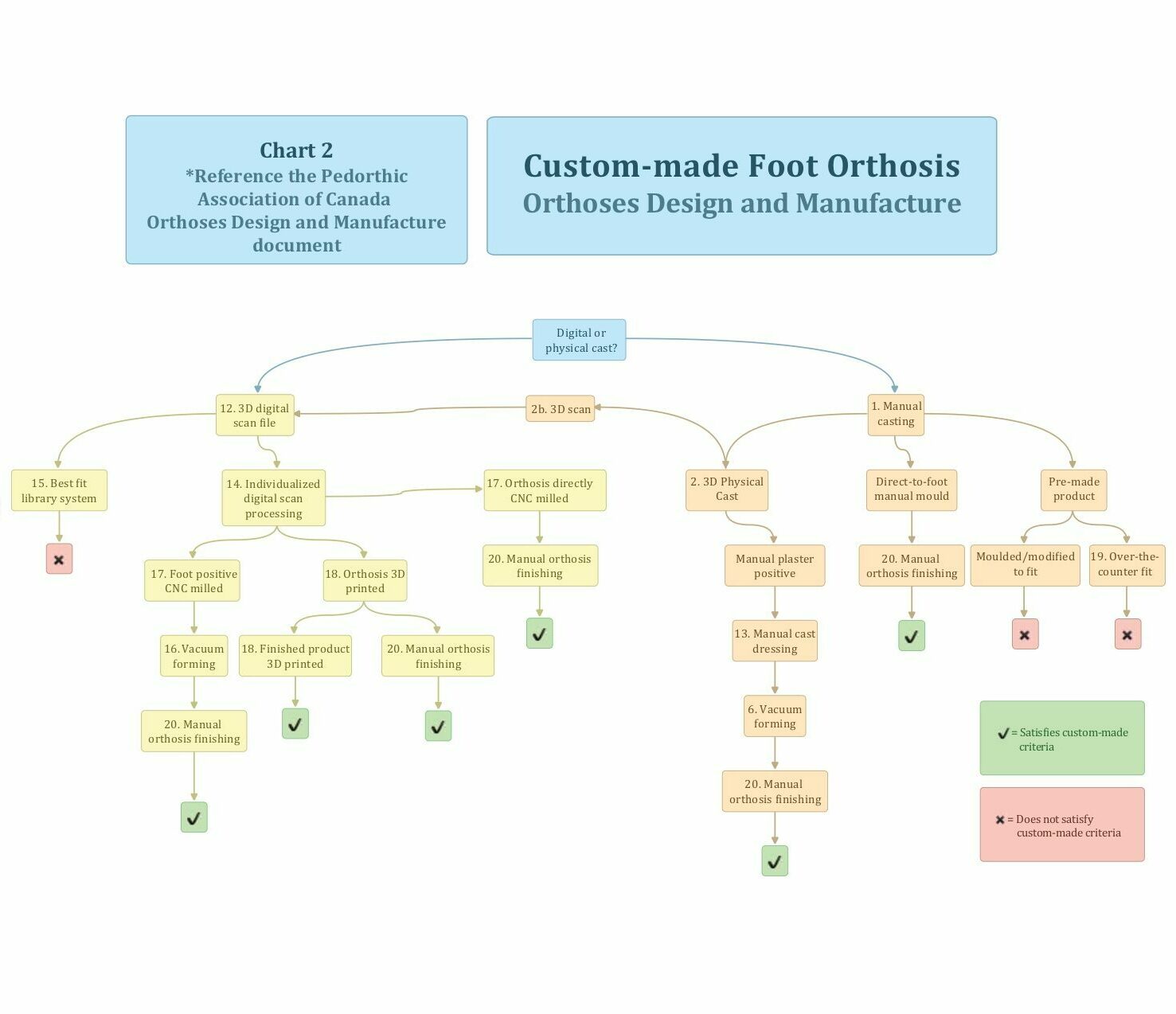
3D Physical Cast: Slipper Casting (Plaster of Paris, Foot Impression Wax, Casting Sock (2)):
- The clinician places the foot in its optimum position.
- A negative cast is taken with plaster, wax, or a polyurethane-embedded sock.
- The cast is used to yield a positive mould for further correction or modification before fabrication of the orthosis.
- This method captures the plantar contour of the foot, as well as the forefoot-to-rearfoot relationship.

Semi-Weight-Bearing Foam Box Casting (3):
- The clinician places the foot in the desired position to achieve optimum posture and carefully controls the posture of the foot during casting.
- A negative cast is taken with a low-density foam block.
- The cast is used to create a positive mould for fabrication of the orthosis. This method captures the contours of the plantar aspect of the foot in a functional posture.
Raw Material Direct-to-Foot Mould (4):
- The clinician chooses thermo-mouldable raw material to use as casting material that will ultimately form part of the finished orthosis.
- This material is heated to the desired temperature in order to make it malleable enough to contour to the structure of the foot.
- The material is then placed on the foot in a non-weight-bearing, semi-weight-bearing, or a full-weight-bearing position.
- The clinician positions the foot to achieve optimum posture and control during casting as the material cools.
- The material (now moulded to the foot) is removed and excess material is cut away.
- Reinforcing layers, padding layers, and other necessary components are then added (e.g., metatarsal pads and posting).
- The raw material is then ground into a shape to become an effective orthotic device.

(Note: Pre-made products (19) where an over-the-counter device is heated and moulded over the physical cast, or where the cast is “best matched” to a pre-made product, are not considered to be custom-made.)

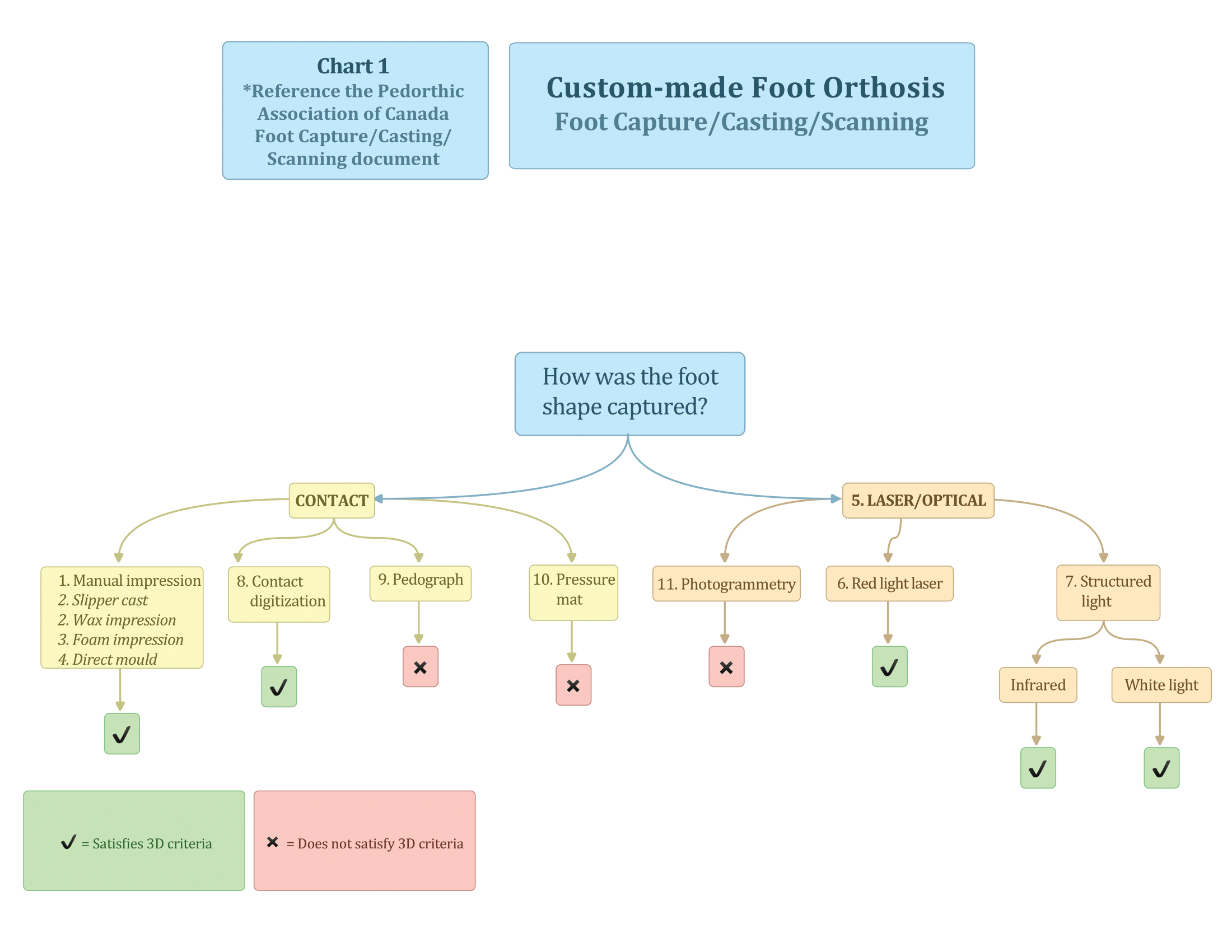
3D Digital Scan (5): Laser/Optical Scanner/Contact Digitization:
If digital technology is used in the provision of custom foot orthoses, the laser or scanning system must create a three-dimensional foot image from points read directly from the foot itself or from a direct model of the foot, such as a plaster slipper cast or foam impression. The scanning technology must not use computer algorithms, extrapolations, or interpretations to calculate shapes and contours from two-dimensional pressure readings, ink impressions, single aspect photographs, or any other two-dimensional methods.
For the purpose of capturing the 3D model of the human foot, there are three main acceptable types of “digital” or “3D scanners” (at present):
- Laser triangulation (red light) (6)
- Structured light (white or infrared light) (7)
- Contact digitization (8)
Laser triangulation uses a laser light to measure the distance between the laser source and the foot to create an accurate model of that foot.
Structured light scanners use the same trigonometric triangulation used in laser scanning, however instead of using a laser light, they project a light pattern onto an object and calculate the distance to the light source.
Contact digitization uses a three-dimensional pin matrix to capture the contours of the plantar aspect of the foot.
Unacceptable Methods
Unacceptable methods that use digital or manual computations to calculate a foot shape include pedographs (9), pressure-sensitive mats (10), and photogrammetry (11).1 These methods do not directly capture the foot’s shape and they require human or digital interpretations.
1Photogrammetry is a method used to create three-dimensional images from a series of two-dimensional photographs. When used appropriately, it can be a highly accurate way to create a three-dimensional image of a foot. That said, this method has not proven to be clinically relevant when applied to casting for custom foot orthoses, as it is an inefficient process that requires significant computing power and clinical time. There are current systems that claim to use photogrammetry when, in reality, they require in-depth computer algorithms to create three-dimensional shapes from a single photograph of any one aspect of the foot. It is for these reasons that PAC recommends photogrammetry be excluded from the acceptable foot capture methods.
Our Position
It is widely accepted that a three-dimensional model of the foot is necessary to produce the most effective custom-made orthosis or shoe possible. There are a variety of different casting techniques available to Canadian Certified Pedorthists, each with its own merits. It is a disservice to the patient to label any single technique as “standard” as it compromises the pedorthist’s ability to choose the best method for a specific patient. Two-dimensional casting is not sufficient because it does not capture the height of the arch and is not a volumetric cast of the entire foot surface.